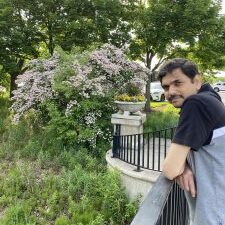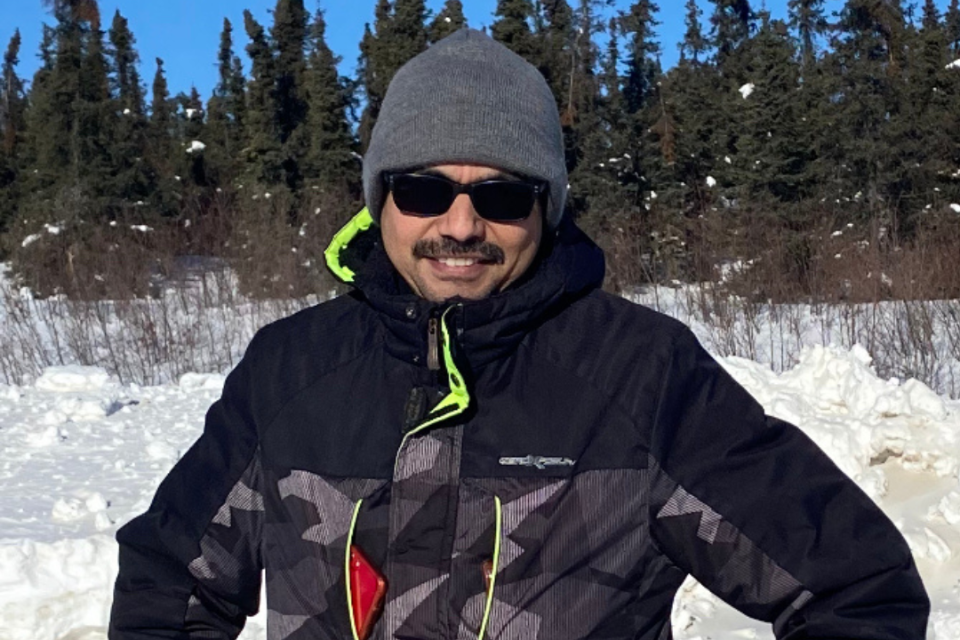
Rohit is an experienced IT professional who has been living in the US since 2006. His job requires him to travel extensively (pre-COVID-19) and he has been able to keep a “clean” diet through all his sojourns. He wishes the healthcare system was more aware of pancreatitis. Based on the missed opportunities in his own journey, he has taken it upon himself to learn more about pancreatitis and help others like him to manage the condition.